Avascular Necrosis of the Femoral Head
Avascular (aseptic) necrosis of the femoral head is a severe chronic progressive disease that develops as a result of impaired blood supply to the femoral head, accompanied by severe pain syndrome, necrosis of a portion of the femoral head and its gradual destruction, significant impairment of hip joint function, and a substantial decrease in the patient's quality of life.
The disease is accompanied by severe pain in the hip joint area. In the initial stages of the disease, the femoral head retains its shape. In later stages, the destruction and deformation of the head occur, leading to the development of secondary osteoarthritis of the hip joint.
The disease primarily affects young people aged 20 to 50 years. Furthermore, the number of patients aged 20 to 30 years has been steadily increasing in recent years. According to literature data, multiple factors can act as a triggering mechanism for the development of avascular necrosis of the femoral head: hip joint trauma, alcohol abuse, prolonged use of hormonal medications, venous stasis, fat embolism, hypercoagulability, and others.
According to our studies, all examined patients with avascular necrosis of the femoral head presented with an impairment of the axial load of the femur, which in turn led to incorrect loading on the head (surprisingly, none of the sources we encountered mentioned impaired axial loading in avascular necrosis of the femoral head). Moreover, 93.5% of the patients (87 out of 93 examined patients) had only an axial load impairment, and we were unable to identify any other triggering factors. In 4.3% (4 patients), approximately 5-7 months before the onset of the first pain sensations in the hip joint area, there were various infectious diseases with an elevation in body temperature above 38ºC lasting for 3-7 days, and 2 patients (2.2%) had a history of prolonged use of hormonal medications.
According to existing treatment standards, in the initial stages of avascular necrosis of the femoral head, core decompression (tunneling) of the femoral head is performed, and analgesics and vasodilators are prescribed. However, unfortunately, the efficacy of such treatment is low, and in the vast majority of cases, the disease progresses and ultimately results in total hip arthroplasty. Orthopedists in Europe and the USA are unanimous in their opinion that the results of endoprosthetics for avascular necrosis of the femoral head cannot be considered satisfactory, especially in young patients, because they require multiple endoprosthesis replacements over their lifetime, and with each replacement, the patient's quality of life decreases. Therefore, it is necessary to search for new approaches to the treatment of avascular necrosis of the femoral head that would allow patients to preserve their native joint.
Since 2002, reports have begun to appear in the literature regarding the successful use of stem cells in the treatment of stages 1-2 of avascular necrosis of the femoral head. Much to our regret, in our country, patients with stages 1-2 of avascular necrosis of the femoral head rarely consult orthopedists. This is explained by the untimely diagnosis of this disease and, consequently, inadequate treatment. Typically, they all initially receive treatment from a neurologist who diagnoses them with osteochondrosis of the lumbosacral spine and conducts the corresponding treatment. And only 6-8 months after unsuccessful treatment (pain in the hip joint area persisted), the patients are referred for an MRI examination of the hip joint area, where avascular necrosis of the femoral head is detected, but usually at stage 2-3 rather than stage 1-2.
At these stages, a bone cavity is already forming in the femoral head, and in some cases, deformation of the head begins. In such situations, standard decompression of the necrotic focus area and the administration of a stem cell suspension are already ineffective.
We have developed a technology for two-stage surgical treatment of avascular necrosis of the femoral head using stem cells. According to this technology, surgical removal of the necrotic bone area from the femoral head and transplantation of stem cells into this area are performed, along with surgical correction of the axial load of the femur. To successfully perform these surgical manipulations, a set of special surgical instruments has been developed and patented.
Following the staged surgical treatment, the load on the femoral head normalizes, blood circulation in the head is restored, and new bone tissue forms in the area of necrosis. All of this contributes to the restoration of the damaged hip joint and its full functioning. This technology has been successfully applied in 57 patients. In all of these patients, their native hip joints were preserved.
Clinical cases
A 32-year-old male patient, Volodymyr, presented with complaints of pain in the right hip joint area associated with avascular necrosis of the right femoral head. The diagnosis of "necrosis of the femoral head" had been established nearly 2 years prior. Conservative management was performed, but it yielded no clinical results. A cavity began to form within the femoral head, and the patient was advised to undergo total hip arthroplasty. Since Volodymyr was serving as a chief mate on a large bulk carrier at that time, replacing the joint with an endoprosthesis meant being medically discharged ashore and terminating his maritime career. Therefore, upon the recommendation of an acquaintance who had previously been treated at our clinic, Volodymyr sought our consultation.
Upon examination, along with necrosis of the anterolateral/superolateral region of the femoral head, a significant inward deviation of the mechanical force acting on the femur was detected. This deviation led to an overload of the joint capsule, an abnormal load distribution on the head itself, and the impairment of its blood supply. When obtaining the medical history, the patient stated that he had not sustained any injuries to the right hip joint. The only factor that could have led to repetitive microtrauma of the joint was the patient's passion for playing volleyball, which he had practiced semi-professionally in his childhood.
We performed restorative staged surgical treatment using autologous stem cells combined with the correction of the axial load of the right femur.
Six months following the surgical treatment, the right femoral head had completely regenerated, the mechanical force acting on the femur was realigned along the axial load axis of the bone, and the pain in the hip joint had disappeared. Volodymyr was able to lead an active lifestyle. An additional 5 months later, he successfully resumed his duties as a chief mate.
Three years post-treatment, Volodymyr presented with no complaints regarding his right hip joint and was preparing to go to sea in his new capacity as a captain.

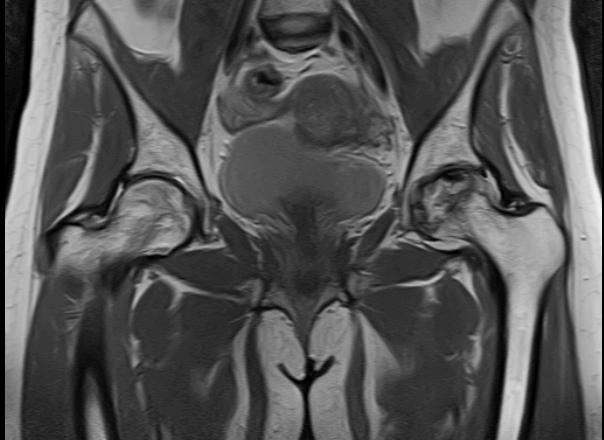
A 52-year-old female patient, Tetiana, presented to our clinic presenting with avascular necrosis of the left femoral head. This diagnosis had been established six months prior, and she was immediately advised to undergo total hip arthroplasty. The patient declined the surgical procedure. Tetiana experienced mild, dull, aching pain in her left hip joint almost continuously, which significantly intensified during ambulation, necessitating the regular use of analgesics.
Upon objective evaluation, MRI slices demonstrated the initial signs of avascular necrosis of the femoral head, presenting as substantial bone marrow edema, a developing focus of necrosis within the head, and pronounced synovitis of the hip joint. Radiographic examination revealed a significant inward deviation of the mechanical force acting on the femur away from the axial load line, as well as a lateral displacement of the femoral head.
Given that the manifestations of the femoral head necrosis were at an initial stage, Tetiana underwent a surgical procedure aimed at correcting the femoral load alignment combined with core decompression (osteotrepination) of the femoral neck and head.
The persistent pain in the left hip joint region completely resolved on the day following the surgery.
Six months postoperatively, when the patient began fully weight-bearing on her left lower extremity, pain in the left hip joint was entirely absent, and the range of motion in the joint had significantly increased.
One year after the treatment, Tetiana presented with no complaints regarding her left hip joint. She led an active lifestyle and moved around frequently. A follow-up MRI examination of the left femoral head revealed bone tissue regeneration within the head, and no signs of synovitis were observed. On follow-up radiographs, the mechanical force acting on the femur was aligned along the axial load axis, and the femoral head was in its correct anatomical position.
